possibility to develop for MSA. PE: within FY2022. However, we have to confirm the thought of TAU for IT asset generation, because Wave collaboration was discontinued and MAPT HDO IT failed
PE within FY2022 would be difficult because of lack of preparation for peptide ligand selection and animal model.
blank
blank
blank
In vitro
Selected 18개 18mer ASO
blank
blank
blank
In vivo
Pilot in vivo -> Select one or two ASO
50% KD (m RNA, at low dose to secure safety margin). Animal model TBD, But SNCA BAC TG (human WT aSyn) is unlikely b/c it does not show pathologic aSn
blank
blank
safety
Focal necrosis is important, Maiko wants to clear this in mice (it is not clear whether this is PE criteria)
blank
blank
blank
note
NHP biodistribution before CN
blank
blank
blank
DMPK MTV
[DMPK MTV]
About ASO vs HDO in TfR construct, team is not excluded ASO and will select ASO or HDO by direct comparison.
Team is currently prioritizing HDO because it generally has long duration in plasma and better biodistribution, and TfR conjugated HDO showed better distribution than TfR conjugated ASO by tool molecules.
Timeline for HDO is not significantly different from that for ASO although some additional works are needed for HDO.
Ryouta Maeda Notes
author / date
notes
Ryouta Maeda 202104
System to IT due to low exposure in CNS. PLAN: no cholesterol ligand. Still system option by transferrin (peptidream, Denali). Expected dosing frequency: Every 1-3 m.
Ryouta Maeda 20200702
Briefly, I think PD marker is total a-syn in CSF and disease progression marker is oligomer a-syn in CSF. If TE marker is needed, SNCA mRNA in plasma NDE is suitable same as MAPT HDO PJ. 20200908: Oligomer aSyn is also important (rather than RT-Quic). Reason: This should be used in vivo assay → 다른 commercial kit 쓰면 될 테니 이건 이유 아닐걸? NDE is important.
Ryouta Maeda 20220713
(in this case it would be important how we differentiate from Ionis IT SNCA ASO, BIIB101. Any thoughts?) We currently think that it might be potency, because there is no report about issues of BIIB101 such as efficacy, safety or duration. But it would be difficult. There are two candidate ASOs from the literature and they showed potent KD efficacy in NHP. Now we are evaluating the KD activity of our HDOs and these IONIS ASOs in model mice by ICV administration to confirm whether our HDOs would show more potent KD activity than that of IONIS’s ASOs at least in mice. (can you briefly help me better understand why the Wave collaboration was discontinued?) We don’t know the reason of discontinuation of Wave collaboration because of firewall. (can you briefly help me better understand why MAPT HDO IT failed?)
MAPT IT HDO PJ could successfully identify the molecule for NHP study. However, we could not appropriately evaluate PK/PD in NHP by IT administration due to technical issues of IT administration at domestic CRO. When we considered the competitiveness with IONIS-MAPTRX and timing of IT asset generation, we decided to focus on BTV asset generation based on business decision.HDO - IT, BTV - IV/SC. To be determined: both in parallel? Or focus on one?아마: If our HDO (IT) could clearly overcome and differentiate from IONIS's ASO, in terms of KD potency in model mice (by ICV administration) -> then we would focus on HDO asset generation.If not -> develop BTV.
20230630 Differentiation Table
date
question / axis
comparator / note
competing area
20230630
Differentiation against IONIS’s clinical candidate, hASO2, on KD depth and duration in model mice (~the end of September 2023)
Does it knock down both WT and mutant aSyn? → it acts on intro, so if the mutation is in exon, then it works.
TE / exposure
↓ aSyn m RNA
Does it knock down all forms (monomeric, phosphorylated, oligomeric?) → yes, because it acts on m RNA. Shall ARNU look at these various forms?
TE / exposure
↓ aSyn m RNA
Regional? Deep structure 잠입어려우니 cortex에 더 효과? Shall ARNU do histology?
protein / neuroprotection
↓ aSyn protein; neuroprotection
Shall ARNU count neurons in various regions? Correlation between these two?
BM
TfR1 PET; ASO
NDE m RNA (from SNCA ASO PRC narrative for PE).
BM
aSyn / imaging readouts
aSyn spreading NHP?; P aSyn; RT Quic; Total aSyn CSF; Asyn PET (QST).
BM
other readouts
Retinal BM?; MIBG?; DATscan; Vmri for LBD.
HDO PET Needs And Questions
item
Needs
Development Stage
HDO PET / ASO PET
ASOs have notoriously poor penetration in deep brain structures (basal ganglia) and other subcortical structures. Lowering of mHTT in patient lumbar CSF as “distal” biomarker of target engagement does not establish origin of this PD effect (spinal cord, cortex, other?). Purpose: visualise drug distribution (not TE, TO). Caveat: it is uncertain how to quantify? How much is enough?
currently similar efforts for ASOs led by Paul McQuade
Paul McQuade: 20200923: this is (theoretically) platform, as long as we use cholesterol-tagging too. And we can start from the step 3.Technical questions:1. Does the plasma/brain ratio of HDO change over time 안 변하면 굳이 pet 필요 없다는 의미 인듯. Is there differential clearance between these tissues, i.e does it clear slower from the brain than plasma. This would allow for Imaging to potentially quantify non-invasively brain accumulation of these constructs.2. Impact chemical modification has on HDO pk profile radioisotope붙여도 pk나 tissue distribution등이 안 변해야 함. Compare modified and non-modified ASO/HDO -> Tomimatsu: 20200923: we are doing cold studies, will get results Jan 2021.3. How long is needed to be able to image the labeled HDOs, this will impact imaging strategy Up to 6 h (F), up to 10 days (I, Zr) or >10 days (Pre-targeting)4. Clinical transability of imaging approach Correct preclinical model Dosimetry
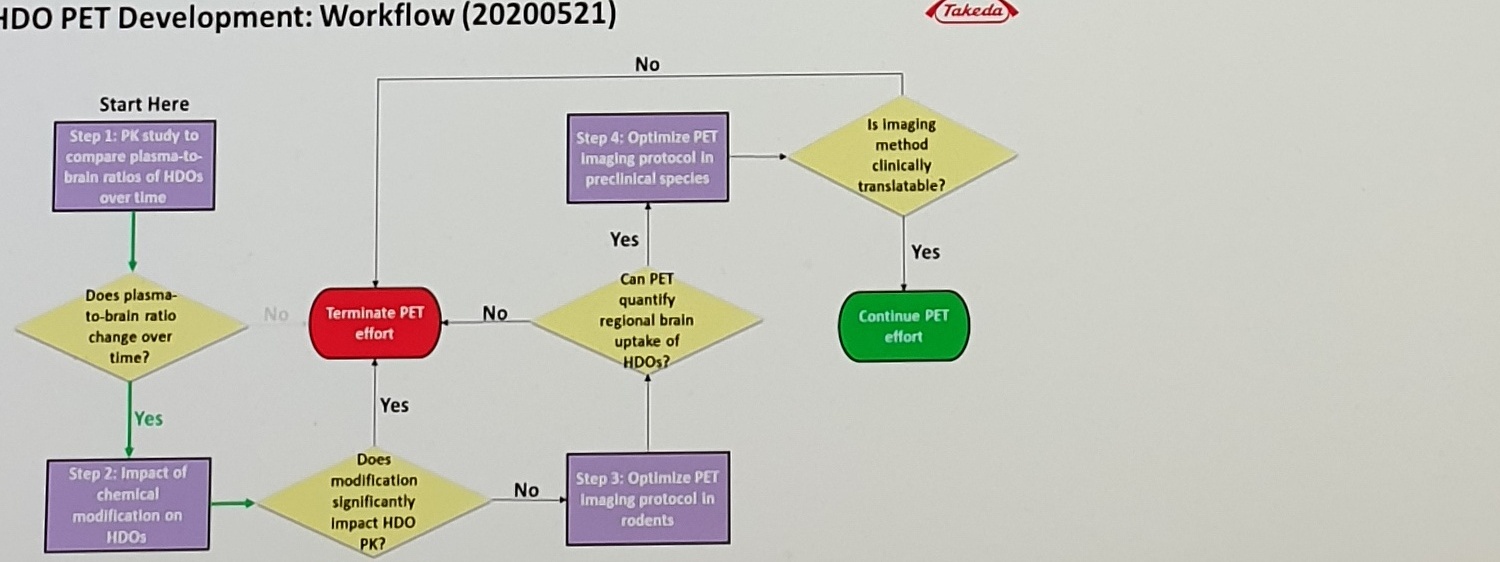
HDO PET Development Workflow
HDO PET Development: Workflow (20200521)Start HereStep 1: PK study to compare plasma-to-brain ratios of HDOs over timeDoes plasma-to-brain ratio change over time?No -> Terminate PET effortYes -> Step 2: Impact of chemical modification on HDOsDoes modification significantly impact HDO PK?No -> Step 3: Optimize PET Imaging protocol in rodentsCan PET quantify regional brain uptake of HDOs?Yes -> Step 4: Optimize PET Imaging protocol in preclinical speciesIs imaging method clinically translatable?Yes -> Continue PET effort
Inferred from the body heading and nav headings; the statusbar also shows nearby SNCA ASO (WAVE) and Executive summary (Ashina, Shuntaro), so the body heading is treated as stronger evidence.
page label
Page 34 of 40
Apple Vision and PaddleOCR agree, but nearby pages may have different statusbar counts depending on the active Word/document state.
SNCA BTV phase table
aSn, m RNA, b/c, NHP biodistribution befoe CN
Preserved visible spelling/spacing where the source itself or OCR is ambiguous.
DMPK MTV
TfR construct, tool molecules, long duration in plasma
Text is readable but line wrapping and spacing are cramped.
Ryouta Maeda 20220713
Ionis IT SNCA ASO, BIIB101; IONIS ASO potency paragraph
High-risk drug/program names and potency claim; visually readable but should be reviewed before KB extraction.
SharePoint URL
SCNA vs SNCA; long View token
URL is wrapped and partly near the page edge; do not normalize without manual check.
Translation table
intro
Could mean intron; source text appears as intro, so it is left unchanged.
Translation table
Vmri for LBD; Asyn PET (QST)
Small text and OCR disagreement on exact capitalization/letters.